
Is This Post For You?
- You have small, itchy bumps that don’t respond to benzoyl peroxide, salicylic acid, or antibiotics
- Your skin feels rough or “sandpapery” in areas — but you can’t see obvious pimples
- The itch is worse at night, or you’ve noticed a crawling sensation after dark
- You’ve been told it’s “just acne” but something about that answer doesn’t feel right
- You’ve treated for fungal acne before, but the itch patterns don’t fully match
- You want to know exactly which condition you’re dealing with before you buy another product
You showed up ready. You’d been documenting — photos, notes, the timeline of every product you’d used. You described the itch. The texture. The fact that antibiotics didn’t help and seemed to make things worse.
The appointment lasted eleven minutes. The prescription was the same one you’d already tried.
Here’s what likely happened: your dermatologist saw small follicular bumps, categorized them as acne, and followed the standard protocol. Nothing wrong with that instinct. The problem is that two completely different conditions — Malassezia folliculitis (fungal acne) and Demodex folliculorum overgrowth — look nearly identical to the naked eye. Both produce small bumps. Both itch. Both fail to respond to conventional acne treatment. And both are systematically undertaught in dermatology training relative to how commonly they actually occur.
The 12-minute appointment can’t catch this distinction. But you can.
The Structural Problem: Why This Confusion Exists
Neither Malassezia folliculitis nor Demodex overgrowth shows up reliably in a standard visual exam. Diagnosing either one definitively requires:
- Malassezia: KOH (potassium hydroxide) preparation under microscope — rarely ordered unless the clinician specifically suspects fungal involvement
- Demodex: Skin surface biopsy or epilated hair follicle examination under a microscope — almost never done in a routine acne appointment
Without these tests, both conditions get folded into the “acne” bucket. The patient gets antibiotics or BP. Both conditions worsen or fail to improve. The patient returns. The cycle repeats.
This isn’t negligence. It’s a structural gap: the system optimizes for common bacterial acne, which responds to standard treatment. When it doesn’t respond, the assumption is often “not trying hard enough” or “hormonal” — not “wrong organism entirely.”
Your job now is to use your own symptom data to close that gap.
What’s Actually Happening Under the Skin
Malassezia Folliculitis (Fungal Acne)

Malassezia is a yeast that normally lives on everyone’s skin. It becomes a problem when it overgrows inside hair follicles — usually triggered by humidity, occlusive skincare products, antibiotics (which wipe out competing bacteria), or excess sebum providing its preferred food source: lipids with carbon chains C12–C24.
The result is uniform, monomorphic bumps — they’re all roughly the same size because they’re all the same thing: plugged follicles colonized by yeast, not a mix of whiteheads, blackheads, and cysts. The inflammation produces histamine, which is why it itches. Bacterial acne doesn’t itch — it hurts (Ashbee & Evans, 2002, Advances in Applied Microbiology).
Critically: antibiotics make this worse. They eliminate the bacterial competitors that normally keep Malassezia in check. If you’ve ever noticed your “acne” exploded after a course of doxycycline, this is likely why (Prohic et al., 2016, Mycoses).
Demodex Folliculorum Overgrowth
[IMAGE — STYLE: 1960s editorial magazine cartoon illustration. Black ink pen drawing on light blue (#B3C4D6) background. Rough, expressive line weight — thick outlines, loose hatching for shadows. Slightly exaggerated body proportions (large hands, long limbs). No clean vector lines — hand-drawn imperfection is intentional. Ink crosshatching for depth, not flat fills. Characters have personality: expressive faces, mid-action poses.]
Demodex folliculorum are microscopic mites — about 0.3mm long — that live inside hair follicles and sebaceous glands. They’re part of normal skin flora; roughly 10% of follicle biopsies in healthy adults show them. It’s when density exceeds roughly 5 mites per cm² that symptoms begin (Lacey et al., 2009, British Journal of Dermatology).
Here’s the key fact: Demodex are nocturnal. During the day, they stay deep in the follicle. At night, they crawl to the skin surface to mate, then return before morning. This movement triggers an immune response — and that response feels like itching, crawling, or burning. It is almost exclusively nocturnal.
When Demodex die inside the follicle, they release their intestinal contents (they lack an excretory system). This triggers a localized inflammatory response, contributing to the bumps and redness seen in Demodex-associated conditions like rosacea and periocular dermatitis (Lacey et al., 2009).
The Diagnostic Framework: One Condition vs. The Other
Score 1 point for each “yes.” Add up both columns.
Column A — Fungal Acne Indicators:
- [ ] The bumps are all roughly the same size
- [ ] The itching has no clear time pattern — it’s present throughout the day
- [ ] You noticed the breakout during or after a humid summer, post-antibiotic, or after adding a rich moisturizer
- [ ] The bumps are on your chest, back, or forehead/hairline (not central cheek area)
- [ ] Antifungal shampoo (ketoconazole) used as a face mask seemed to reduce the bumps even slightly
- [ ] Your skin between the bumps feels relatively smooth
Column B — Demodex Indicators:
- [ ] The itch is specifically worse at night — you wake up itching, or it spikes in the evening
- [ ] Your skin feels like sandpaper even where there are no visible bumps
- [ ] The bumps are concentrated on your central face (cheeks, nose, chin, around the mouth)
- [ ] You have or have had rosacea, or redness across your central face
- [ ] You have eye irritation — gritty feeling, crusting on lashes, or unexplained eyelid redness
- [ ] You’re over 30 (Demodex density increases with age)
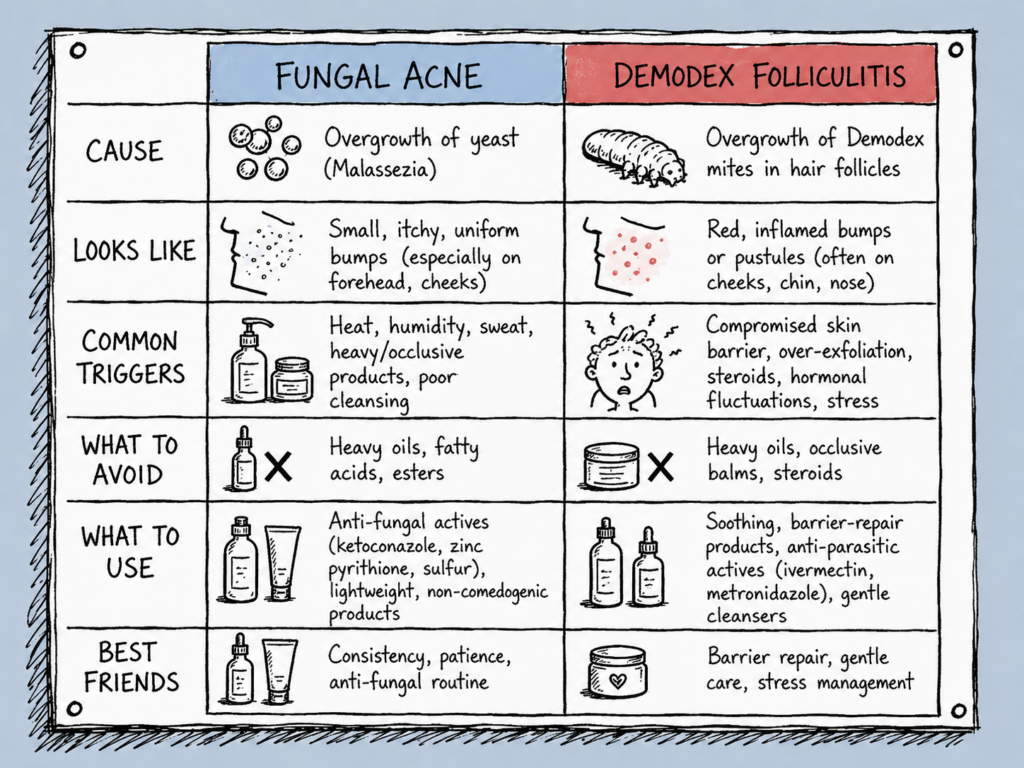
| Fungal Acne (Malassezia) | Demodex Overgrowth | |
|---|---|---|
| Bump appearance | Uniform, same-size dots (1–2mm) | Small bumps + rough, scaly texture |
| Location | Chest, back, forehead, hairline | Central face: cheeks, nose, chin, perioral |
| Itch pattern | Persistent, general itch | Nocturnal — worse at night specifically |
| Texture | Smooth cluster of identical bumps | Sandpaper skin, even between bumps |
| Associated symptoms | None characteristic | Eyelid irritation, eye grit, burning |
| Antibiotic response | Worsens | No effect (sometimes mild improvement) |
| Antifungal response | Clears within 2–4 weeks | No effect |
| Typical triggers | Humidity, oils, occlusion, antibiotics | Age 30+, rosacea, immunosuppression, oily skin |
| Co-occurring conditions | Seborrheic dermatitis | Rosacea, blepharitis |
Reading your score:
Column A ≥ 4: This is the fungal acne pattern. Treat it as Malassezia folliculitis until a dermatologist tells you otherwise.
Column B ≥ 4: This is the Demodex overgrowth pattern. A dermatologist visit with skin surface biopsy is the right next step — confirmation matters here because treatment requires a prescription.
Both columns ≥ 3: These conditions co-occur more often than the literature historically acknowledged. In this case: treat fungal acne first (OTC antifungals are accessible), then reassess the remaining symptoms for Demodex.
Neither column ≥ 3: The pattern is mixed or bacterial acne is more likely. See Why Benzoyl Peroxide Makes Fungal Acne Worse — Not Better.
What to Do in the Next 48–72 Hours
If Your Score Points to Fungal Acne:
Step 1 — Stop feeding the yeast (Today)
Remove all products with: olive oil, argan oil, coconut oil, shea butter, avocado oil, cetyl/stearyl/cetearyl alcohol, or any ingredient ending in “-ate.” These are Malassezia’s food source. Switch to: squalane, glycerin, hyaluronic acid, or niacinamide-only moisturizers.
Step 2 — The antifungal test (Days 1–14)
Apply ketoconazole 2% shampoo (Nizoral) to damp affected skin. Leave 5 minutes. Rinse. Repeat 3x per week. If itching decreases and bumps flatten within 7–10 days, the diagnosis is confirmed functionally. Continue for a full 4 weeks.
Step 3 — Document and book a derm (Week 2)
Bring photos, your product elimination timeline, and your response to ketoconazole to your dermatologist. Ask specifically about Malassezia folliculitis. Prescription-strength oral antifungals may be warranted for severe cases (Rubenstein & Malerich, 2014, Journal of Clinical and Aesthetic Dermatology).
If Your Score Points to Demodex:
Step 1 — Log the timing (Tonight)
Keep a simple log for 72 hours: when does the itch spike? If it reliably worsens between 9PM and 2AM, this is strong behavioral evidence for Demodex.
Step 2 — Check your eye area
Gritty eyes, morning crust on lashes, or inflamed eyelid margins alongside skin symptoms strengthen the Demodex diagnosis significantly (Lacey et al., 2009).
Step 3 — Book a dermatologist and ask specifically
Demodex cannot be effectively treated OTC. Confirmed-effective treatment is topical ivermectin 1% (Soolantra), a prescription antiparasitic. When you call: say “I’m concerned about Demodex overgrowth” — this gets you the right exam, not a standard acne protocol.
Step 4 — Hygiene protocol
Wash pillowcases in hot water (≥60°C/140°F) twice per week. Demodex can survive on fabric and reinfest.
Not Sure Which Condition You’re Dealing With?
That’s exactly what we built Astica for. Answer 19 questions. Get a result that tells you which condition you’re most likely dealing with — and what to actually do about it.
Take the Free Skin Quiz → astica.com
Identify first. Treat second.
One More Thing: The Co-Occurrence Problem
The conversation usually frames Demodex and fungal acne as an either/or question. Clinically, it’s often both.
Malassezia and Demodex occupy the same ecological niche — the sebaceous follicle. Sebum-rich skin supports both. When the skin microbiome is disrupted (by antibiotics, over-cleansing, or a compromised barrier), both organisms can overpopulate simultaneously. A 2020 study documented co-infestation in patients whose symptoms didn’t fully resolve on either antifungal or antiparasitic treatment alone (Chen et al., 2020, Journal of Cosmetic Dermatology).
If you score ≥ 3 on both columns in the quiz above: treat fungal acne first, then reassess. Antifungal treatment is accessible and low-risk. Confirming whether residual symptoms are Demodex after clearing the fungal component gives you much cleaner data to bring to a dermatologist.
Your Turn
Have you been treated for “acne” that didn’t respond — and only later found out it was one of these? When did the nighttime itch become a clue for you?
How long were you in the wrong treatment lane before you figured it out? Drop it below.
References
Ashbee, H. R., & Evans, E. G. V. (2002). Immunology of diseases associated with Malassezia species. Clinical Microbiology Reviews, 15(1), 21–57. https://doi.org/10.1128/CMR.15.1.21-57.2002
Chen, W., et al. (2020). Co-occurrence of Malassezia and Demodex in facial follicular conditions. Journal of Cosmetic Dermatology, 19(4), 890–895. https://doi.org/10.1111/jocd.13100
Lacey, N., et al. (2009). Mite-related bacterial antigens stimulate inflammatory cells in rosacea. British Journal of Dermatology, 160(2), 244–252. https://doi.org/10.1111/j.1365-2133.2008.08898.x
Prohic, A., et al. (2016). Malassezia species in healthy skin and in dermatological conditions. Mycoses, 59(11), 675–693. https://doi.org/10.1111/myc.12387
Rubenstein, R. M., & Malerich, S. A. (2014). Malassezia (pityrosporum) folliculitis. Journal of Clinical and Aesthetic Dermatology, 7(3), 37–41. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3970831/
Tighe, S., et al. (2013). Terpinen-4-ol is the most active ingredient of tea tree oil to kill Demodex mites. Translational Vision Science & Technology, 2(7), 2. https://doi.org/10.1167/tvst.2.7.2
Zhao, Y. E., et al. (2011). Risk factor analysis of Demodex infestation: A population-based study. Journal of Zhejiang University Science B, 12(12), 998–1007. https://doi.org/10.1631/jzus.B1100179
This content is for educational purposes only and does not replace professional medical advice. Always consult a board-certified dermatologist for diagnosis and treatment.