Why Benzoyl Peroxide Makes Fungal Acne Worse
Is This Post For You?
- You’ve been using benzoyl peroxide for 4+ weeks with zero improvement
- Your bumps got worse — or multiplied — after starting BP
- Your skin is dry and flaking, but the bumps keep appearing
- Everything itches more when you sweat
- A dermatologist told you to “give it more time” — and more time hasn’t helped
- You’ve started to wonder if BP is part of the problem, not the solution
You did everything right.
Booked the appointment three weeks in advance. Showed up without makeup so they could actually see your skin. Brought photos of your forehead in different lighting to document what was happening.
After a 12-minute consultation, your dermatologist handed you a prescription for benzoyl peroxide and said: “Give it six weeks.”
Six weeks later, your skin is drier, the bumps have multiplied, and you’re Googling at 2AM. You find a Reddit thread from someone describing your exact skin — same texture, same itching, same complete non-response to BP — and you start to wonder if you’ve been treating the wrong thing entirely.
You have. Or at least, you might.
The Structural Problem: Why This Keeps Happening
Here’s what nobody tells you when you walk out of that appointment: benzoyl peroxide is the correct first-line treatment for roughly 85% of acne cases. Starting there isn’t a mistake — it’s statistically sound clinical decision-making under time pressure.
The problem is the other 15%.
A standard 12–15 minute dermatology visit doesn’t include a KOH test (the 5-minute in-office test that identifies fungal infection). Without it, Malassezia folliculitis — fungal acne — looks identical to bacterial acne under visual examination. Same uniform papules, same forehead distribution, same patient complaint: “I keep breaking out and nothing is working.”
The system isn’t set up to catch this. Insurance often won’t cover “exploratory” fungal testing when the chart says “acne.” Dermatology residencies spend significantly more hours on acne vulgaris than on Malassezia folliculitis — a condition that accounts for up to 40% of treatment-resistant acne cases (Rubenstein & Malerich, 2014).
So the prescription gets written. You follow it faithfully. And the condition gets worse.
That’s not your failure. That’s a structural gap — and understanding it is the first step to getting out of it.
What Benzoyl Peroxide Actually Does
BP is genuinely effective for bacterial acne. Understanding why helps explain why it backfires so completely on fungal acne.
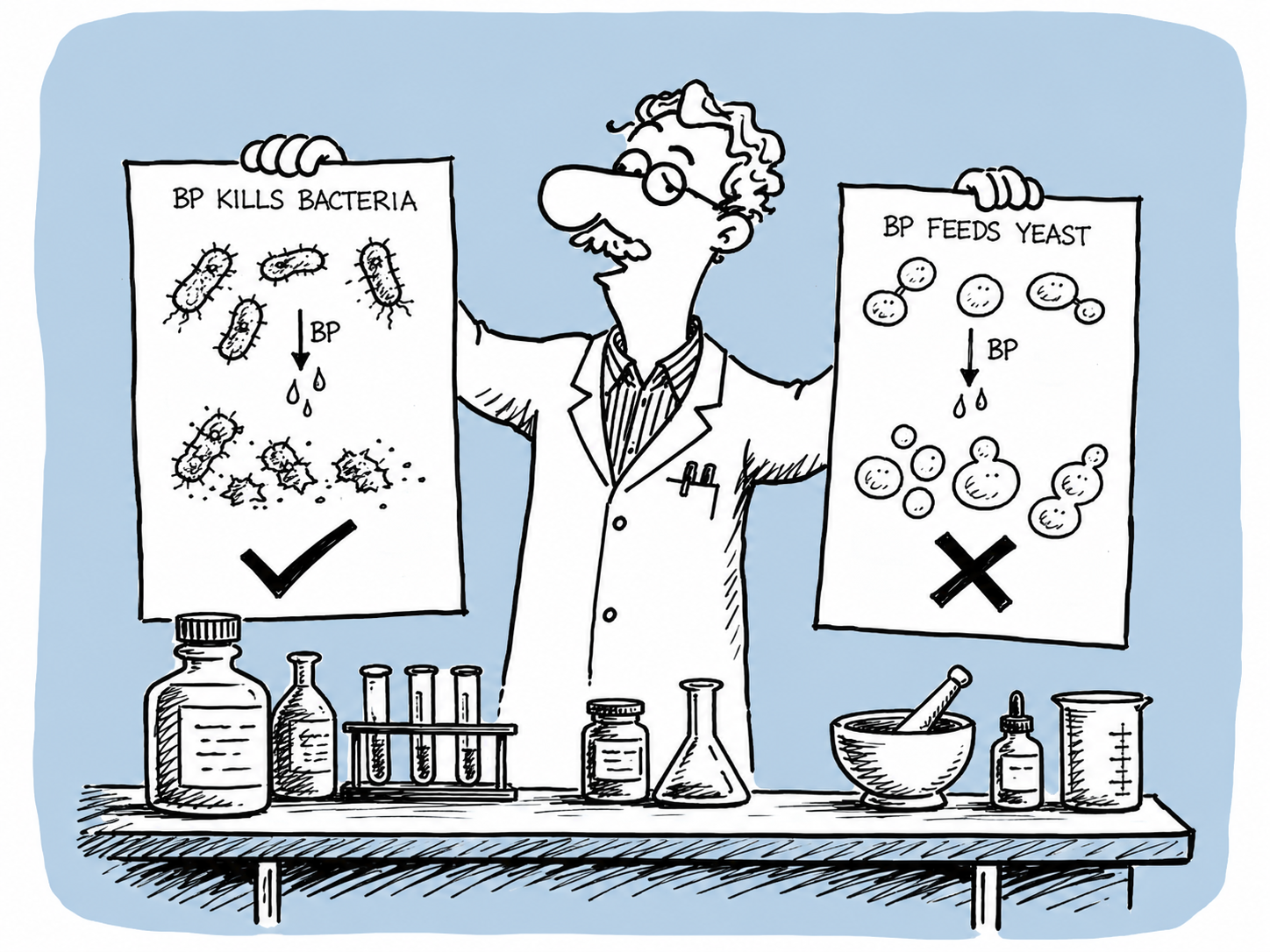
Benzoyl peroxide works by releasing oxygen into hair follicles. Cutibacterium acnes — the bacteria responsible for traditional acne — is anaerobic. It cannot survive in an oxygen-rich environment. BP kills it directly and efficiently.
For bacterial acne, this is exactly what you want.
For fungal acne, it’s a different story entirely. Malassezia is a yeast, not a bacterium. Oxygen doesn’t touch it. But BP does three other things that actively make the situation worse:
It strips your skin barrier. The protective acid mantle — the slightly acidic film that keeps your skin pH around 4.5–5.5 — gets disrupted by repeated BP use. When your barrier is compromised, Malassezia has easier access to the follicles it’s colonizing.
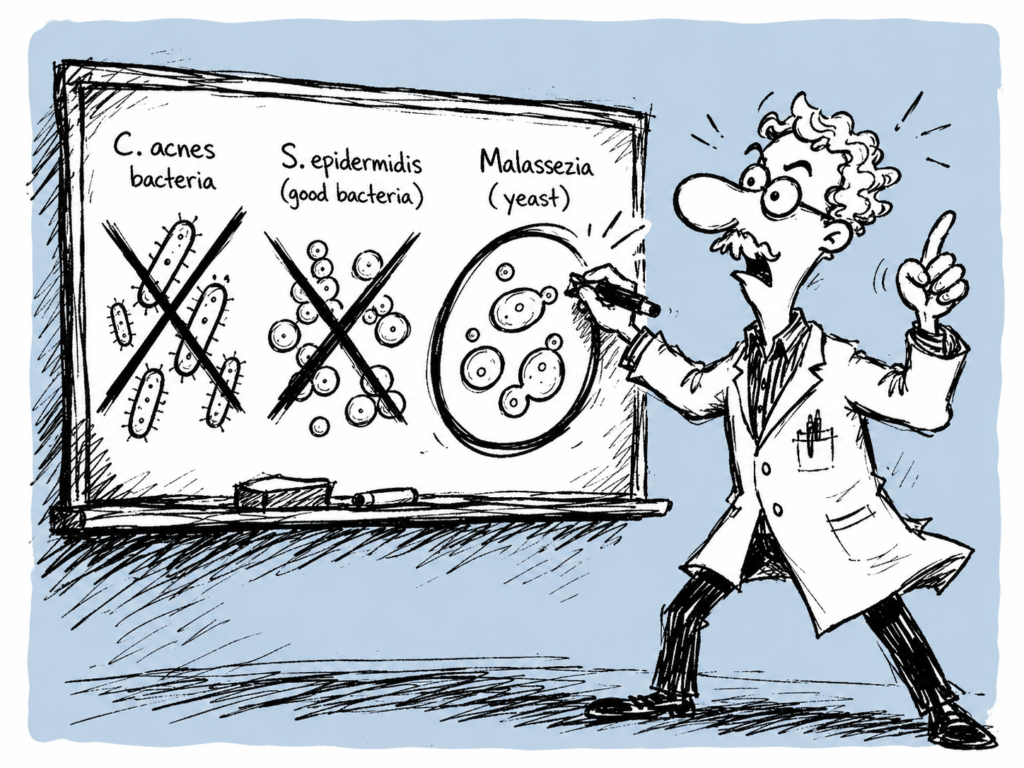
It eliminates bacterial competition. Your skin hosts a complex microbiome. Staphylococcus epidermidis and other commensal bacteria naturally suppress Malassezia overgrowth by competing for resources. BP kills them alongside C. acnes, clearing the field for yeast to expand.
It creates a drier, more alkaline environment. Malassezia actually thrives when skin pH rises above 5.5. The dryness and pH disruption caused by BP creates conditions the yeast prefers.
Think of your skin as a garden with multiple species. Benzoyl peroxide is a broad-spectrum herbicide. For bacterial acne, it kills the weed you’re targeting. For fungal acne, it kills everything that was competing with the weed — and the weed spreads.
Gupta, A. K., et al. (2004). Skin diseases associated with Malassezia species. Journal of the American Academy of Dermatology, 51(5), 785–798.
The Antibiotic Problem: When It Gets Even Worse
The BP-to-antibiotic pipeline is the most common path from “bad” to “significantly worse” for undiagnosed fungal acne patients.
The typical timeline looks like this:
Weeks 1–4: BP isn’t working. Skin is getting drier. Bumps are multiplying.
Week 5–6: You go back. Your dermatologist prescribes oral antibiotics — doxycycline or minocycline — for the “treatment-resistant acne.”
Weeks 6–8: Your skin actually improves. The antibiotics are working.
Weeks 9–12: It comes back. And it’s worse than it was before.
Here’s what happened: the antibiotics killed C. acnes and temporarily reduced inflammation. But they also eliminated the bacterial populations that were keeping Malassezia in check. With bacterial competition gone, the yeast population expands rapidly. Skin pH shifts from its natural acidic range toward neutral — exactly where Malassezia thrives.
Research confirms that oral antibiotic use is one of the most consistent triggers for Malassezia folliculitis flares. The temporary improvement you saw wasn’t the acne getting better — it was the bacterial component resolving while the fungal component quietly took over.
Cogen, A. L., et al. (2008). Skin microbiota: a source of disease or defence? British Journal of Dermatology, 158(3), 442–455.
How to Know If BP Is Making Your Condition Worse
Not every non-response to BP means fungal acne. Use this checklist to read your own pattern.
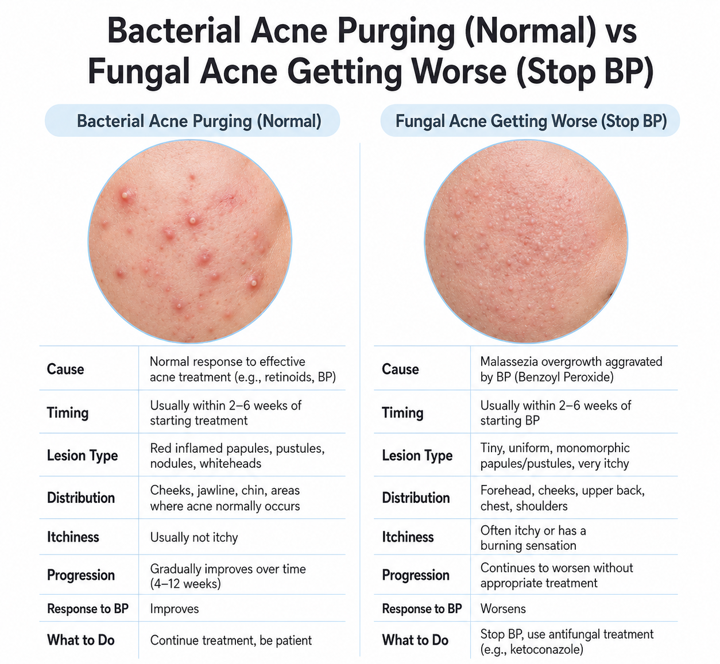
Signs BP is working (bacterial acne purge — normal):
- ✓ Peaks at weeks 2–3, then clearly improves
- ✓ Existing bumps surface and resolve
- ✓ New bumps scattered, not clustered
- ✓ Better by week 6
Signs BP is making it worse (stop — reassess):
- ✗ New bumps appearing in identical clusters after starting BP
- ✗ Getting worse past week 4, not better
- ✗ Bumps are uniform size — all the same, no mixed presentation
- ✗ Itching increased since starting BP, especially when sweating
- ✗ Skin is flaking and dry, but bumps keep multiplying
- ✗ Antibiotic course helped briefly, then it came back worse
The 8-week rule: If you are past week 8 on BP and your skin is not measurably better, this is not a purge. A purge resolves. This is the wrong treatment.
The 2-Week Test: What to Do Right Now
If your checklist answers point toward fungal acne, here is your action plan.
Week 1: Stop everything
Pause BP. Pause retinoids. Pause exfoliating acids.
Use only:
- A gentle, sulfate-free cleanser
- A fungal-safe moisturizer — hyaluronic acid, glycerin, or squalane base. No oils high in oleic or palmitic acid (olive oil, argan oil, shea butter).
Observe: Does the itching decrease within 48 hours? Does your skin feel calmer? That signal alone is diagnostically useful.
Week 2: Test the antifungal theory
Add one of the following:
Ketoconazole 2% (Nizoral shampoo used as a face mask):
Apply to damp skin. Leave on 5 minutes. Rinse. Use twice weekly.
Zinc pyrithione 2% wash (Noble Formula or DermaHarmony):
Lather on face for 2 full minutes. Rinse. Safe for daily use.
Track: If itching decreases within 3–5 days and new bumps stop appearing within 7–10 days, the pattern is fungal. Stop treating it like bacterial acne.
How to Have a Better Dermatologist Conversation
Don’t go back saying “I think I have fungal acne.” Go back with this:
“I’ve tracked my symptoms closely. The bumps are all uniform in size, they itch especially when I sweat, and they actually got worse after antibiotics. I’ve had no measurable improvement after 8 weeks on BP. Could we do a KOH test to rule out Malassezia folliculitis before adjusting treatment?”
This works because you’re presenting clinical observations, not a self-diagnosis. You’re asking to rule something out — not insisting on a conclusion. You’re using the correct medical terminology. And you’re giving your dermatologist actionable data they can work with.
A KOH test takes 5 minutes in office and confirms or rules out fungal infection definitively. If yours declines without explanation, a second opinion is appropriate.
Not Sure Which Condition You’re Dealing With?
Answer 19 questions. Get a result that tells you what you’re most likely dealing with — and what to actually do about it.
Take the Free Skin Quiz → astica.com
Identify first. Treat second.
Your Turn
Two questions — drop your answers below:
- How many weeks were you on BP before you suspected something was wrong? And what was the specific moment that made you question it?
- Did antibiotics help temporarily and then make things worse? That timeline is one of the clearest signals we see.
References
Rubenstein, R. M., & Malerich, S. A. (2014). Malassezia (pityrosporum) folliculitis. The Journal of Clinical and Aesthetic Dermatology, 7(3), 37–41. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3970831/
Gupta, A. K., Batra, R., Bluhm, R., Boekhout, T., & Dawson, T. L. (2004). Skin diseases associated with Malassezia species. Journal of the American Academy of Dermatology, 51(5), 785–798. https://doi.org/10.1016/j.jaad.2003.12.034
Cogen, A. L., Nizet, V., & Gallo, R. L. (2008). Skin microbiota: a source of disease or defence? British Journal of Dermatology, 158(3), 442–455. https://doi.org/10.1111/j.1365-2133.2008.08437.x
Gaitanis, G., Velegraki, A., Mayser, P., & Bassukas, I. D. (2013). Skin diseases associated with Malassezia yeasts: facts and controversies. Clinics in Dermatology, 31(4), 455–463. https://doi.org/10.1016/j.clindermatol.2013.01.012
American Academy of Dermatology. (2023). Acne: Diagnosis and treatment. https://www.aad.org/public/diseases/acne/diagnosis-treatment
This content is for educational purposes only and does not replace professional medical advice. Always consult a board-certified dermatologist for diagnosis and treatment.