Is This Post For You?
- You have tiny, uniform bumps on your forehead that have been there for weeks — or months
- You’ve tried benzoyl peroxide or salicylic acid and nothing changed (or it got worse)
- The bumps itch, especially when you sweat
- Your skin looks “textured” in certain lighting but the bumps don’t really have heads
- A dermatologist told you it’s acne — but standard acne treatment isn’t working
- You’re starting to wonder if something is being missed
You’ve been doing everything right.
Double cleansing every night. The BHA toner everyone swears by. You booked the dermatologist appointment three weeks out, showed up without makeup so they could really see your skin, even took photos in natural light to document what was happening.
Twelve minutes later, you walked out with a benzoyl peroxide prescription and instructions to “give it six weeks.”
Six weeks pass. The bumps are still there. Some days they look angrier. You go back. “Give it more time. Try adding a retinoid.”
Three months in, you’re still Googling at 2AM — “tiny bumps forehead won’t go away” — reading through Reddit threads from people describing your exact skin, wondering if you’re losing your mind.
You’re not. And your skin isn’t “difficult.”
The problem isn’t that the treatment isn’t strong enough. The problem is that you may be treating the wrong condition entirely.
Why This Keeps Happening: The Structural Problem
Here’s what nobody explains when you leave that appointment: a 12-minute consultation is not designed to catch conditions that look identical to acne vulgaris under visual examination.
Dermatologists are working within a system that makes certain diagnoses nearly impossible to catch in a standard appointment. Here’s why:
Time. A 12–15 minute visit is industry standard. In that window, a physician must take history, examine your skin, and write a prescription. There’s no time for a differential diagnosis workup on what looks like a common presentation.
Statistics. Cutibacterium acnes — the bacteria behind traditional acne — accounts for roughly 85% of inflammatory acne cases. Starting with the most statistically likely diagnosis isn’t bad medicine. It’s how clinical decision-making works under time constraints.
Visual limitation. Without magnification, cultures, or a KOH test, fungal acne, bacterial folliculitis, and Demodex folliculitis look essentially identical to bacterial acne. Uniform red papules, same distribution, same patient complaint.
Training gaps. Malassezia folliculitis receives significantly less attention in dermatology residencies than its actual prevalence warrants. It’s frequently taught as a condition seen in immunocompromised patients — not as a common cause of “treatment-resistant acne” in otherwise healthy adults.
The result: patients cycle through months of ineffective treatment, spending money and damaging their skin barrier, while the underlying condition goes unaddressed.
This is not a failure of your dermatologist. It’s a structural failure — and it’s exactly the problem ASTICA is built to address.
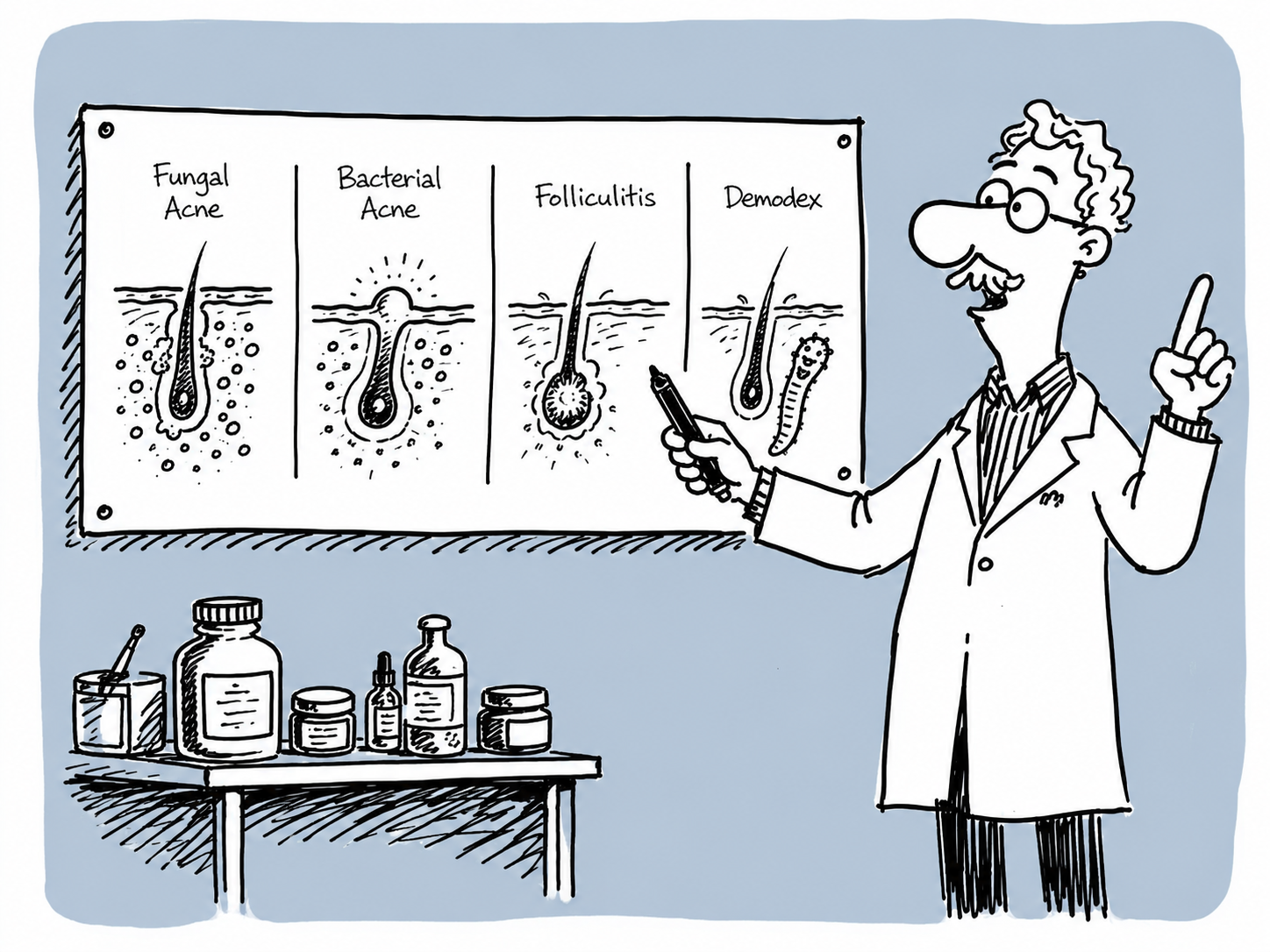
The Four Conditions That Look Identical on Your Forehead
Your forehead bumps could be one of four things. Each looks nearly the same to the naked eye. Each requires a completely different treatment. Getting this wrong doesn’t just mean the treatment won’t work — some treatments for one condition actively make another worse.
![[ALT TEXT: Dr. Aster illustrating the four types of forehead bumps on a whiteboard]](https://labs.astica.com/wp-content/uploads/2026/05/image-1024x683.png)
Condition 1: Fungal Acne (Malassezia Folliculitis)
What it actually is: Not a bacteria. Not a comedone. Malassezia is a yeast — part of your normal skin flora — that overgrows when conditions shift and triggers inflammation inside hair follicles.
What you see:
- Uniform 1–2mm papules, all the same size
- Clustered in crops — they appear together, not scattered
- Smooth, dome-shaped, no visible head
- Flesh-colored to slightly pink
- Concentrated on the forehead, hairline, and sometimes upper back or chest
The defining feature: It itches. Fungal acne itches — especially when you sweat, when you’re warm, or when you apply certain moisturizers. Bacterial acne is painful when pressed. Fungal acne itches without being touched.
Why it happens: Malassezia is lipophilic — it feeds on fatty acids. When it metabolizes specific lipids (particularly oleic, palmitic, and lauric acid), it produces inflammatory byproducts that rupture the follicle wall from the inside. Your immune system responds with a papule.
Common triggers: humid environments, occlusive moisturizers with heavy oils, oral antibiotics (which kill bacterial competition), prolonged sweating, high-sugar diets.
What makes it worse: Benzoyl peroxide, antibiotics, and most conventional acne treatments. These don’t affect yeast and may actively feed the overgrowth by eliminating bacterial competition.
Gaitanis, G., et al. (2012). The Malassezia genus in skin and systemic diseases. Clinical Microbiology Reviews, 25(1), 106–141.
Condition 2: Bacterial Acne (Acne Vulgaris)
What it actually is: The condition your dermatologist is almost certainly treating. Cutibacterium acnes bacteria proliferate inside clogged pores, triggering an immune response.
What you see:
- Mixed presentation — tiny blackheads alongside larger papules, pustules, or cysts all at once
- Scattered distribution, not uniform clusters
- Variety of sizes in the same area
- Visible “head” on pustules
- White, black, or red lesions depending on stage
The defining feature: It hurts. Inflammatory acne is tender to the touch. Pressing a papule causes pain.
What works: Benzoyl peroxide, salicylic acid, retinoids, oral antibiotics for inflammatory cases.
Leyden, J. J., & Del Rosso, J. Q. (2011). Oral antibiotic therapy for acne vulgaris. Journal of Clinical and Aesthetic Dermatology, 4(2), 40–47.
Condition 3: Bacterial Folliculitis
What it actually is: A bacterial infection of individual hair follicles, most commonly Staphylococcus aureus.
What you see:
- Larger than fungal acne — 3–5mm
- Isolated bumps, not uniform clusters
- Visible hair in the center of the bump
- Pus-filled top with a red, inflamed base
- Warm and tender to touch
The defining feature: You can see the hair coming out of the center. The bump feels like a small boil — warm, tender, sometimes throbbing.
What works: Topical or oral antibiotics, benzoyl peroxide wash, addressing the friction or contamination source.
Laureano, A. C., et al. (2014). Facial bacterial infections: folliculitis. Clinics in Dermatology, 32(6), 711–714.
Condition 4: Demodex Folliculitis
What it actually is: Demodex folliculorum — microscopic mites that live inside hair follicles. Everyone has them. The problem occurs when populations spike and trigger inflammation.
What you see:
- Rough, sandpaper texture more than visible bumps
- Concentrated around nose, cheeks, chin, and forehead
- Pink or red background with subtle scaling
- Tiny pustules at the base of eyebrow hairs on close inspection
The defining feature: Worse at night. Demodex mites emerge from follicles after dark — this triggers the characteristic nighttime itching and crawling sensation.
What works: Tea tree oil 5%, ivermectin cream (prescription), sulfur-based treatments.
Zhao, Y. E., et al. (2011). Sociodemographic characteristics and risk factor analysis of Demodex infestation. Journal of Zhejiang University Science B, 12(12), 998–1007.
The Diagnostic Framework: Read Your Own Pattern
Step 1: Look
| Observation | Points to |
|---|---|
| All bumps are the same size (1–2mm) | Fungal Acne |
| Mix of sizes — some tiny, some large | Bacterial Acne |
| Visible hair in the center of bumps | Bacterial Folliculitis |
| Skin feels rough/sandpaper, bumps barely visible | Demodex |
| Bumps appear in identical clusters | Fungal Acne |
| Bumps scattered randomly | Bacterial Acne |
Step 2: Feel
| Sensation | Points to |
|---|---|
| Itchy — especially when sweating or warm | Fungal Acne |
| Painful / tender when pressed | Bacterial Acne or Folliculitis |
| Itching or crawling worse at night | Demodex |
| No pain, just texture | Fungal Acne or Demodex |
Step 3: Trace Your Triggers
| Trigger | Points to |
|---|---|
| Started or worsened after antibiotics | Fungal Acne |
| Flares before menstrual cycle | Bacterial Acne (hormonal) |
| Worse after hot yoga, sauna, humid weather | Fungal Acne |
| Appeared after switching to a richer moisturizer | Fungal Acne |
| Started after shaving, waxing, or helmet use | Bacterial Folliculitis |
| Worse after heavy face creams applied at night | Demodex |
Step 4: Check Treatment History
| Treatment Response | Points to |
|---|---|
| Benzoyl peroxide made it noticeably worse | Fungal Acne |
| Antibiotics helped briefly, then it came back worse | Fungal Acne |
| Salicylic acid did nothing | Fungal Acne or Demodex |
| BP is helping, slowly | Bacterial Acne or Folliculitis |
Reading Your Results
Mostly Fungal Acne signals:
Uniform bumps + itching + worsened by antibiotics or rich moisturizers = fungal acne pattern. Treat it as a Malassezia pattern until proven otherwise. Stop piling on acne actives that clearly aren’t working. Switch to antifungal-safe products.
Mostly Bacterial Acne signals:
Mixed bump sizes + painful lesions + partial response to BP = bacterial acne. Standard treatment is appropriate. Consider hormonal factors if it clusters on the jaw and flares monthly.
Mostly Bacterial Folliculitis signals:
Bumps with visible hair + warmth + tenderness = folliculitis. Identify the friction or contamination source. Benzoyl peroxide wash applies here too.
Mostly Demodex signals:
Sandpaper texture + nighttime itching + no response to conventional treatment = Demodex pattern. A dermatologist visit is warranted to confirm and prescribe ivermectin if needed.
Split answers:
Mixed patterns are common. Fungal acne and Demodex frequently co-occur. In mixed cases, treat the dominant pattern first, then reassess.
The Ingredient Trap
If you suspect fungal acne, your moisturizer might be actively feeding the yeast.
Ingredients that feed Malassezia — check your labels:
- High-oleic oils: olive oil, argan oil, avocado oil, sweet almond oil, marula oil
- Fatty acids/esters: lauric acid, myristic acid, palmitic acid, stearic acid
- Butters: shea butter, cocoa butter
- Esters ending in “-ate”: isopropyl myristate, isopropyl palmitate
- Fermented ingredients: galactomyces, sake, rice water
Ingredients that are safe:
- Squalane (from sugarcane) — Malassezia cannot metabolize it
- Hyaluronic acid, glycerin, niacinamide
- Linoleic-dominant oils: grapeseed, rosehip, hemp seed
- MCT oil (caprylic acid / C8 only)
What to Do in the Next 48 Hours
Step 1: Stop everything that isn’t working (Today)
Pause all active treatments — benzoyl peroxide, retinoids, exfoliating acids.
Use only:
- A gentle, sulfate-free cleanser
- A fungal-safe moisturizer (squalane, glycerin, or hyaluronic acid base)
Observe: Does itching decrease within 48 hours? That’s a strong signal.
Step 2: Test the antifungal theory (Days 3–14)
Option A — Ketoconazole 2% (Nizoral used as face mask): Apply to damp skin, leave 5 minutes, rinse. Twice weekly.
Option B — Zinc pyrithione wash (Noble Formula or DermaHarmony): Lather on face, leave 2 minutes, rinse. Daily use is fine.
If itching decreases within 3–5 days and new bumps stop appearing within 7–10 days: you have enough signal to stop treating it like ordinary acne. Full stop.
Step 3: Audit your products
Check every current product against the Malassezia-feeding ingredient list. One product with shea butter or argan oil in the top 5 ingredients can undo two weeks of antifungal work.
Step 4: Talk to your dermatologist — differently
Don’t say “I think I have fungal acne.” Say this:
“I’ve been tracking my symptoms. The bumps are uniform size, they itch when I sweat, and they got worse after my last antibiotic course. I’ve had zero response to benzoyl peroxide over 8 weeks. Could we do a KOH test to rule out Malassezia folliculitis before adjusting treatment?”
You’re presenting observations, not a self-diagnosis. You’re using clinical terminology. You’re asking to rule something out — not demanding a conclusion. Good dermatologists respond well to this.
Not Sure Which Pattern Fits You?
Answer 19 questions. Get a result that tells you what you’re most likely dealing with — and what to actually do about it.
Identify first. Treat second.
Your Turn
- How long have your forehead bumps been there, and what treatments have you already tried?
- Do the bumps itch — and when is it worst?
- Did anything in the trigger list above match your timeline?
References
Gaitanis, G., Magiatis, P., Hantschke, M., Bassukas, I. D., & Velegraki, A. (2012). The Malassezia genus in skin and systemic diseases. Clinical Microbiology Reviews, 25(1), 106–141. https://doi.org/10.1128/CMR.00021-11
Rubenstein, R. M., & Malerich, S. A. (2014). Malassezia (pityrosporum) folliculitis. The Journal of Clinical and Aesthetic Dermatology, 7(3), 37–41. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3970831/
Leyden, J. J., & Del Rosso, J. Q. (2011). Oral antibiotic therapy for acne vulgaris. Journal of Clinical and Aesthetic Dermatology, 4(2), 40–47. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3108317/
Laureano, A. C., Schwartz, R. A., & Cohen, P. J. (2014). Facial bacterial infections: folliculitis. Clinics in Dermatology, 32(6), 711–714. https://doi.org/10.1016/j.clindermatol.2014.02.009
Zhao, Y. E., et al. (2011). Sociodemographic characteristics and risk factor analysis of Demodex infestation. Journal of Zhejiang University Science B, 12(12), 998–1007. https://doi.org/10.1631/jzus.B1100079
American Academy of Dermatology. (2023). Acne: Diagnosis and treatment. https://www.aad.org/public/diseases/acne/diagnosis-treatment
This content is for educational purposes only and does not replace professional medical advice. Always consult a board-certified dermatologist for diagnosis and treatment.